How to Manage an Achilles Tendon Rupture
Do you have an Achilles Tendon Rupture?
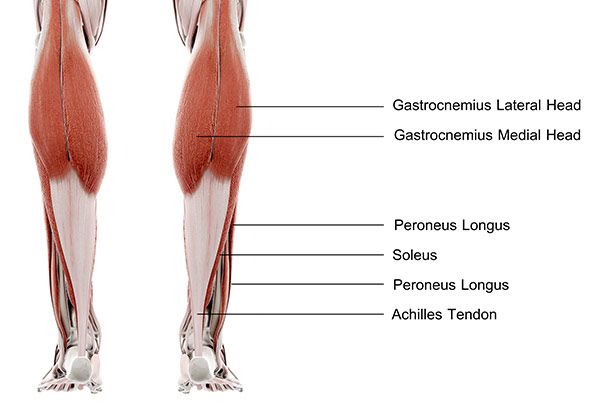
The Achilles tendon is the largest and strongest tendon in the human body. It connects the calf muscles in the back of the leg to the heel bone. When the calf muscles contract (flex) the Achilles tendon pulls on the heel, causing the foot to point. This movement gives us the ability to stand on our toes, and as it is so strong allows us to run and jump as required.
The Achilles tendon is super strong, and it has been shown that it can bear loads exceeding over 900 kilograms during running.
However, due to the high loads that can be suddenly put through the tendon, it is at risk of tearing or rupturing – particularly during sports that require a quick change of direction or start/stop.
What is an Achilles Tendon Rupture?
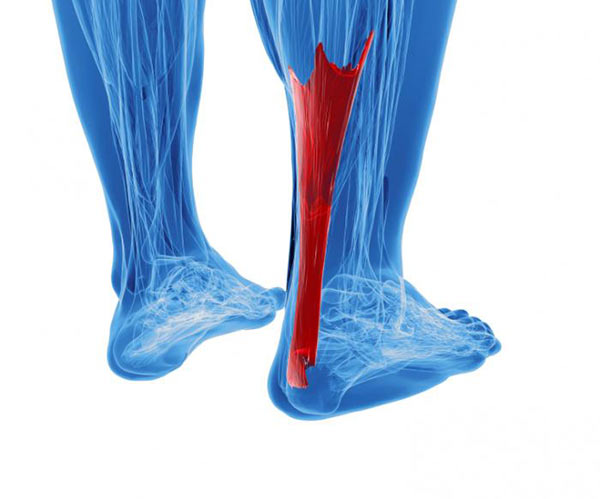
An Achilles tendon rupture is a complete or partial tear that occurs when the tendon is stretched beyond its capacity. Complete tears are more common than partial tears. Forceful jumping or pivoting, or sudden accelerations of running, can overstretch the tendon and cause a tear.
An injury to the tendon can also result from falling or tripping. Achilles tendon ruptures are most often seen in ‘weekend warriors’ – typically, middle-aged people participating in sports in their spare time. Less commonly, illness or medications, such as steroids or certain antibiotics, may weaken the tendon and contribute to ruptures.
I have personally seen 3 Achilles tendon ruptures on a squash court – in each instance the player concerned suddenly looked behind to see what had hit the back of their leg!
Signs and Symptoms of Achilles Tendon Rupture
Although it’s possible to have no signs or symptoms with an Achilles tendon rupture, most people have:
- The feeling of having been kicked in the calf
- Pain, possibly severe, and swelling near the heel
- An inability to bend the foot downward or “push off” the injured leg when walking
- An inability to stand on the toes on the injured leg
- A popping or snapping sound when the injury occurs
Risk Factors for Achilles Tendon Rupture:
Factors that may increase your risk of Achilles tendon rupture include:
- Age: The peak age for Achilles tendon rupture is 30 to 40.
- Sex: Achilles tendon rupture is up to five times more likely to occur in men than in women. Some studies report of 10:1 male: female incidence
- Recreational sports: Achilles tendon injuries occur more often during sports that involve running, jumping, and sudden starts and stops — such as soccer, basketball and tennis.
- Steroid injections: Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures.
- Certain antibiotics: Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture.
- Obesity: Excess weight puts more strain on the tendon.
Diagnosing an Achilles Tendon Rupture:
If you think you may have ruptured your Achilles tendon, is it important to get it diagnosed quickly. Most people I know of attended ED as no medical practitioners were on-hand at the time of injury – the pain and loss of function were severe. In saying that, I have had a few people limp into the clinic here not aware that their Achilles was ruptured.
An Achilles tendon rupture is relatively easy to diagnose by a trained practitioner, generally:
- There is an inability to stand up on the toes/marked weakness of ankle plantarflexion (pointing the foot). *Sometimes people are still able to stand on their toes with the use of other ankle/calf muscles.
- Positive calf squeeze test – the ankle/foot doesn’t flex with the leg is relaxed and the calf is squeezed by the practitioner
- There can be a palpable gap in the tendon – normally 3-6 cm above the heel bone
- The foot ‘hangs’ in a different way when lying on stomach and relaxed.
Ultrasound can assess the injury, with MRI being the gold-standard scan. Imaging may or may not be required.
An orthopaedic surgeon or sports physician should confirm the injury and management plan.
How should an Achilles Tendon Rupture be managed?
There are two pathways to go down when managing an Achilles tendon rupture – surgery or conservative management. Both have their own set of pros and cons.
Conservative management:
Conservative management of a ruptured Achilles tendon generally involves initial immobilisation of the ankle in a cast or functional brace. Initially, the foot ankle is placed in full plantarflexion (pointing toes/foot away). The aim of this is to restore contact between the two ends of the tendon to facilitate healing. There is great variation in treatment regimes, but generally the foot is moved towards neutral by way of adjusting the cast/brace over a period of 8-12 weeks.
Pro’s:
- No surgery!
Con’s:
- Some studies show a higher re-rupture rate in conservatively managed achilles tendon ruptures (2-6% higher rate)
- Some studies have shown that the achilles tendon may heal longer than if it is surgically fixed. This may cause the calf to be weaker in the long term.
Surgical management:
The two ends of the ruptured tendon can be ‘tied’ together through the use of surgery. There are a number of different ways to do this – ‘open’ surgery is often not required, and mini-open or percutaneous surgery can be used with less risk.
As per the conservative management, the foot is placed in a cast/boot initially post-surgery with the ankle/foot pointing away. Slowly the foot is progressively moved back towards neutral over a period of generally 6-10 weeks.
Pro’s:
- Lower re-rupture rate reported in some studies (2-6%)
Con’s:
- Surgical risk: risk of infection, bleeding, abnormal scarring, issues with anaesthetic etc.
So is conservative or surgical management preferred for Achilles Tendon Rupture?
A recent meta-analysis of the literature showed that surgical treatment of Achilles tendon ruptures reduces the risk of re-rupture compared with nonoperative treatment. However, re-rupture rates are low and differences between treatment groups are small (risk difference 1.6%).
Operative treatment results in a higher risk of other complications (risk difference of 3.3%). Their conclusion was that the final decision on the management of acute Achilles tendon ruptures should be based on patient-specific factors and shared decision making!
More definitive research is required!
The decision needs to be based on the fitness/activity levels of the affected person, the age, general health, and goals in regards to returning to function/timeframes.
From what I have seen, my viewpoint is that most Achilles tendon ruptures can be managed conservatively if they are diagnosed quickly and correct treatment is undertaken straight away.
Surgery may be required if there is a delay between injury and correct management (>1 week), or if it is found the tendon has retracted too far (too big a gap between the two ends of the ruptured tendon).
Physiotherapy management of Achilles Tendon Rupture:
Above all, well-managed physiotherapy-led rehabilitation is essential for a good outcome post Achilles tendon rupture – with either surgery or conservative management.
Unfortunately, initial progress is slow. The foot is slowly returned to a neutral position over 2-3 months post-injury. Patience is required while the tendon heals.
Following this gradual strengthening of the lower limb is required, and best done and progressed under physiotherapy supervision – re-rupture of the tendon can happen if too much force is placed through the tendon before it is ready!
Jenna has provided excellent tips on calf strengthening here.
There is variability in the timeframes before return to sport/normal activity – though usually a minimum of 6 months is required before the tendon/patient is ready to get back to normal.
References:
www.sciencedaily.com/releases/2017/11/171120085811.htm
www.mayoclinic.org/diseases-conditions/achilles-tendon-rupture/symptoms-causes/syc-20353234
Wilkins R, Bisson, LJ. Operative Versus Nonoperative Management of Acute Achilles Tendon Ruptures: A Quantitative Systematic Review of Randomized Controlled Trials. Am J Sports Med. 2012 Sep;40(9):2154-60
Ochen Y, Beks RB et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ 2019;364:k5120
Gulati V, Jaggard M, Al-Nammari SS, Uzoigwe C, Gulati P, Ismail N, Gibbons C, Gupte C. Management of achilles tendon injury: a current concepts systematic review. World journal of orthopedics. 2015 May 18;6(4):380.
Munegato D, Gridavilla G et al. Mini open versus open repair techniques in Achilles tendon rupture: clinical and isokinetic evaluation. Muscles Ligaments Tendons J. 2017 Jul-Sep; 7(3): 554–561.
Liechti DJ, Moatshe G et al. A Percutaneous Knotless Technique for Acute Achilles Tendon Ruptures. Arthrosc Tech. 2018 Feb; 7(2): e171–e178.
Brukner P, Kahn, K. Clinical Sports Medicine (3rd Ed). 2007 Sydney